A plain-language guide to every medication in a fertility cycle — what each one does, when it's given, and the brands you'll actually see in Thailand.
Adapted and translated from an article by Dr. Patsama Vichinsartvichai, MD, EFOG-EBCOG, EFRM-ESHRE/EBCOG, FACOG, MClinEmbryol.
Every fertility patient — and even people who've already been through IVF — knows that medication names can feel overwhelming. This guide walks you through every drug we use, grouped the way we actually use them in clinic.
Treatment breaks down into two halves: the egg-collection cycle (stimulation, ovulation blockade, and the trigger shot) and the embryo-transfer cycle (uterine-lining preparation). The medications differ, but the goal is the same — the right cavity at the right moment, receiving the right embryo.
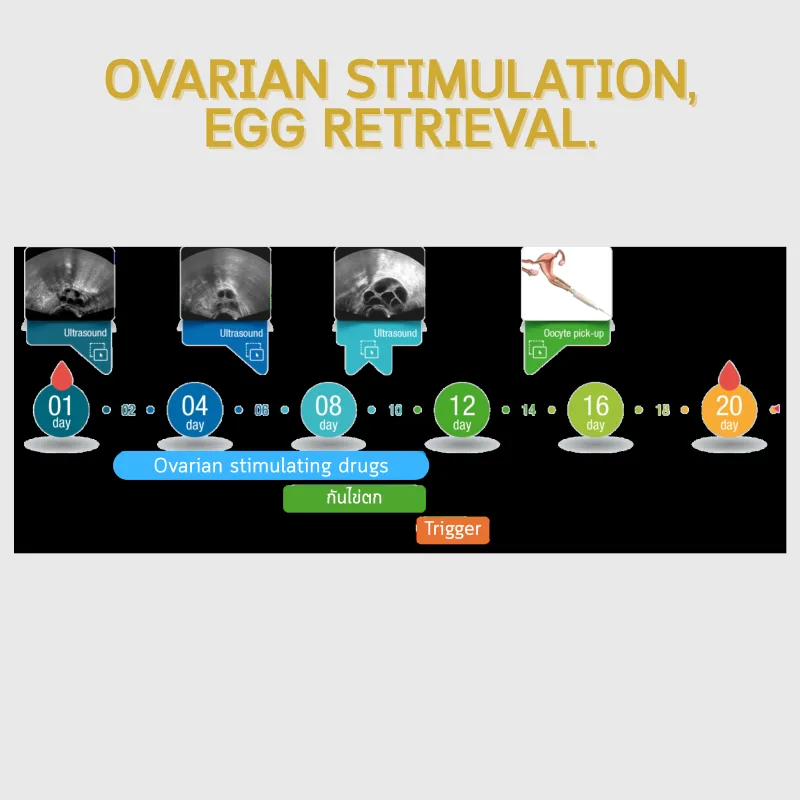
The goal here is to grow more than one follicle in a single cycle so we have several eggs to fertilize. Stimulation drugs come in two forms: oral tablets and injectables.
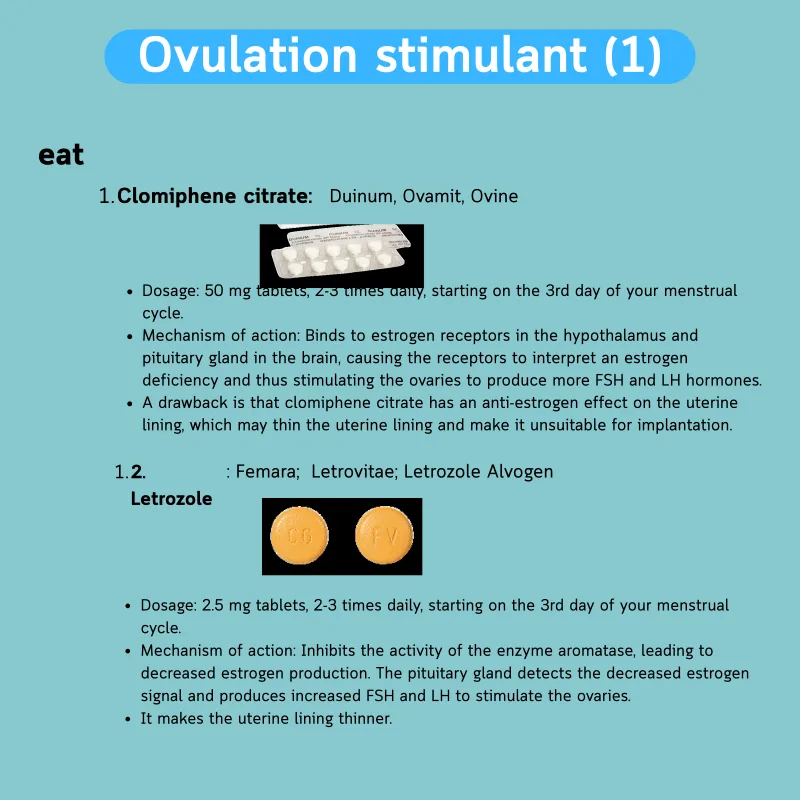
Used mostly when someone will conceive naturally, in PCOS patients whose ovaries aren't ovulating, in IUI cycles, or in mild/minimal-stim IVF. Two are widely used in Thailand:
Binds estrogen receptors in the hypothalamus, tricking the brain into raising FSH — which drives follicle growth.
Downside: also blocks estrogen at the uterine lining, so the endometrium may be thinner than normal. Ovulation can happen 25–50% earlier or later than expected, and effects can carry over into the next cycle.
50 mg tablets · 1–3 tabs/day × 5 days from cycle day 3–5 · Brands: Ovinum, Ova-mit, DuinumBlocks the aromatase enzyme that converts testosterone into estrogen. Lower estrogen prompts the brain to release more FSH — again driving follicle growth. Originally a breast-cancer drug; research supports off-label use in stimulation.
Downside: same thin-endometrium risk as clomiphene, but usually milder.
2.5 mg tablets · 1–3 tabs/day × 5 days · Brands: Femara, Letrovitae, Letrozole Alvogen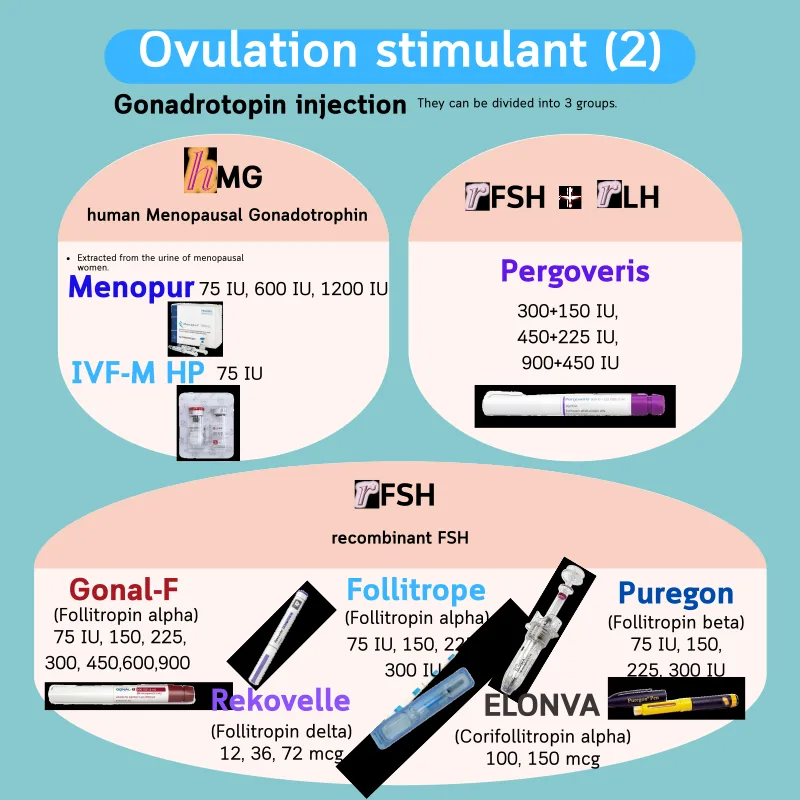
For IVF/ICSI where we want many follicles, injectable FSH is the workhorse. Modern products fall into three families:
Manufactured from Chinese hamster ovary cell line. Prefilled pen with adjustable dose — you can dial the dose up or down, but you cannot dial back once dispensed.
Prefilled pens: 300 · 450 · 900 IU · IUI: 50–100 IU/day · IVF: 150–300 IU/day (up to 450 IU when needed)Same active ingredient as Gonal-F, delivered as prefilled single-use syringes — no dose adjustment; you use exactly what's in the syringe.
Prefilled syringes: 75 · 150 · 225 · 300 IUAlso from Chinese hamster ovary line. Available as vials (50, 100 IU — mix yourself) or as prefilled cartridges (300, 600 IU) that need Puregon's own pen. Dial forward only — do not reverse.
Vials: 50 · 100 IU · Cartridges: 300 · 600 IUManufactured from a human fetal retinal cell line, so the molecule is closer to native human FSH. Dosing is in micrograms, not IU. Adjustable prefilled pen.
Prefilled pens: 12 · 36 · 72 mcgPurified from postmenopausal women's urine. Contains FSH plus hCG-driven LH activity — useful when a patient truly needs LH added. Multidose vials let the doctor prescribe custom doses.
Vials: 75 IU · Multidose: 600 IU · 1200 IU · custom orders 37.5 – 300 IUAnother hMG. In Thailand only the 75 IU vial is available (some countries also carry an IVF-M HP 600 IU multidose).
Vials: 75 IUA modified FSH fused with hCG's tail — one injection lasts 7 days, so daily jabs during the first week aren't needed.
Prefilled syringe: 100 · 150 mcgThe only combination product with both r-hFSH (follitropin alfa) and r-hLH (lutropin alfa) in the same pen — for patients who genuinely need supplemental LH.
Prefilled pens: 300+150 · 450+225 · 900+450 IU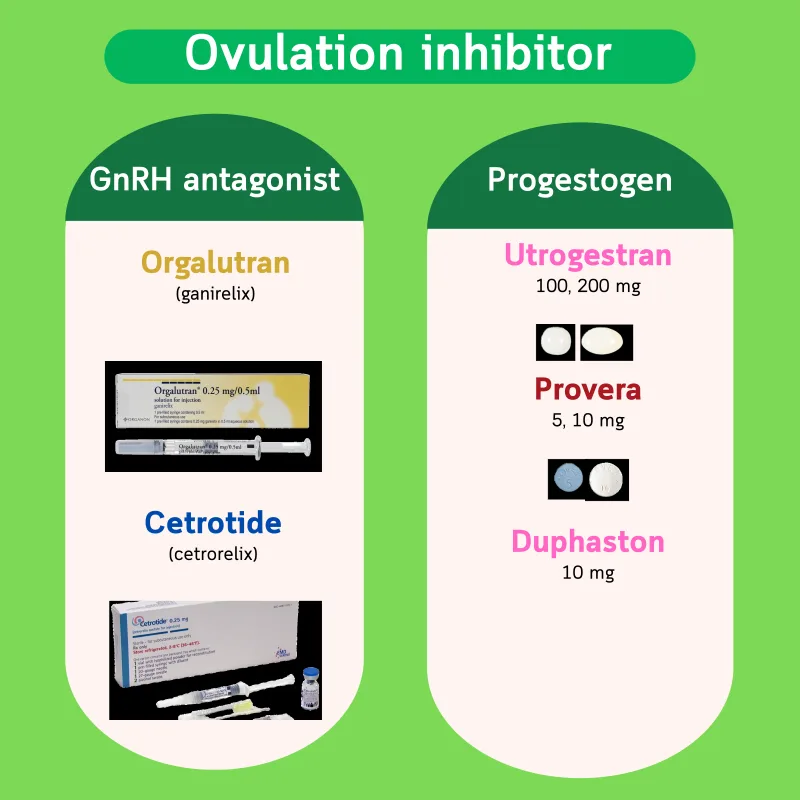
Once follicles grow, estrogen rises and the brain wants to release an LH surge — which would trigger ovulation before we can retrieve the eggs. We prevent this with one of two families:
Directly blocks GnRH receptors, so no LH surge can be triggered. Prefilled syringe — pull out, inject, done.
250 mcg (0.25 mg) prefilled syringeSame drug class. Comes as vial + water — reconstitute before injecting.
250 mcg (0.25 mg) vialProgesterone blocks the LH surge just like it does in birth control. In PPOS we use progestogens to prevent premature ovulation. Common choices: Provera, Duphaston, Utrogestan, Cerazette, and Visanne (dienogest).
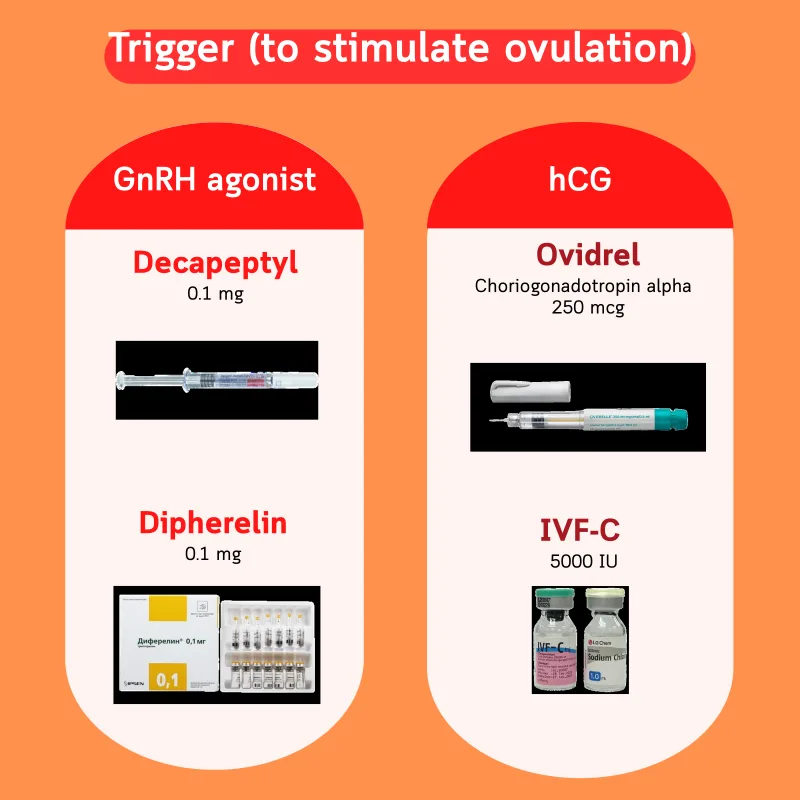
Once the follicles reach the right size, we need to send a signal so the eggs finish maturing and become collectable. Two options:
Prefilled syringe — quick surge of LH from the body's own pituitary. Useful in patients at high risk of OHSS.
0.1 mg prefilled syringeSame agonist mechanism, delivered as vial + reconstitution.
0.1 mg vialhCG binds the same LH receptor and stays active longer than native LH — so it's a reliable "single-shot" way to trigger ovulation.
250 mcg prefilled penPurified hCG from urine. Vial — inject intramuscularly. (Older brand Pregnyl is no longer sold in Thailand.)
5000 IU vial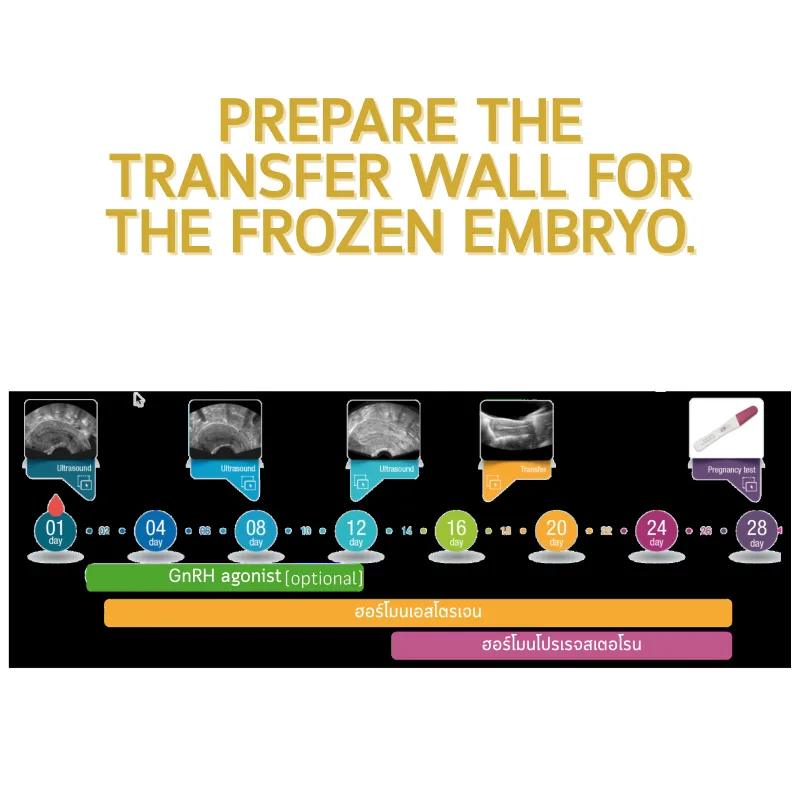
For frozen embryo transfers (FET) we typically use just two hormones: estrogen in the first half of the cycle to thicken the endometrium, then progesterone in the second half to make it receptive.

Available as tablets, transdermal gels/patches, and vaginal preparations. Route matters: oral estrogen gets filtered by the liver first, so only 10–20 % of an oral 100 mg dose reaches the uterus. Transdermal (skin) delivers 70–80 %.
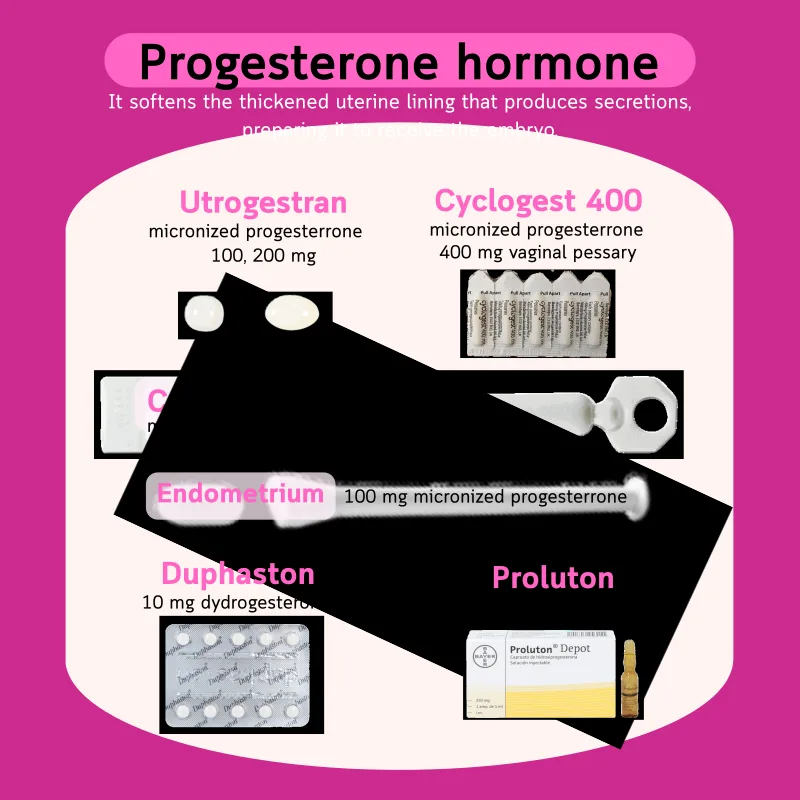
Oral progesterone gets metabolized so heavily it can cause nausea and dizziness, so we mostly use vaginal preparations and intramuscular injections instead. Dydrogesterone (Duphaston) is a synthetic that avoids those side effects and can be taken by mouth.
Sometimes prescribed before a cycle to regulate menses or to suppress a leftover cyst. Common Thai-market brands: Marvelon, Mercilon, Diane-35, Yasmin, Yaz, Belara, Natazia, Microgynon-30ED.
For endometriosis or chocolate cysts — often used before an IVF cycle to calm active disease.
Dopamine agonist for hyperprolactinemia. High prolactin can suppress ovulation.
For PCOS patients with insulin resistance — helps restore ovulation and improves stimulation response.
500 · 850 mg · 1000 mg XRThis article is an English adaptation of the Thai-language essay "ยาที่ใช้ในการรักษามีบุตรยาก IUI IVF ICSI มีอะไรบ้าง? แต่ละตัวทำงานอย่างไร?" by Dr. Patsama Vichinsartvichai, MD, EFOG-EBCOG, EFRM-ESHRE/EBCOG, FACOG, MClinEmbryol. Brand and dosing information reflect products sold in Thailand at the time of writing and can change; always follow your prescribing physician's directions.
Keywords: gonadotropin · IVF · ICSI · GnRH · LH · FSH · estradiol · progesterone · GnRH agonist · GnRH antagonist · dipherelin · triptorelin · ganirelix · cetrorelix · orgalutran · cetrotide · gonal-f · puregon · rekovelle · follitrope · menopur · IVF-M · IVF-C · Ovidrel